Our articles are not designed to replace medical advice. If you have an injury we recommend seeing a qualified health professional. For more information see out Terms and Conditions.
The idea for today’s email came from a podcast from our friends at the Physio Network. I’d recommend having a listen, it’s a great episode with Dr Melinda Smith.
Dr Smith discusses some recent research, and I wanted to share that with you as part of our recent series of newsletters on Plantar Heel Pain (PHP). So we’ll explore this study, implications for practice and then the bigger picture with taping.
Kinesiotaping versus low-dye for plantar heel pain – García-Gomariz et al. (2024)
Here’s a graphic summary with a brief overview of the study:
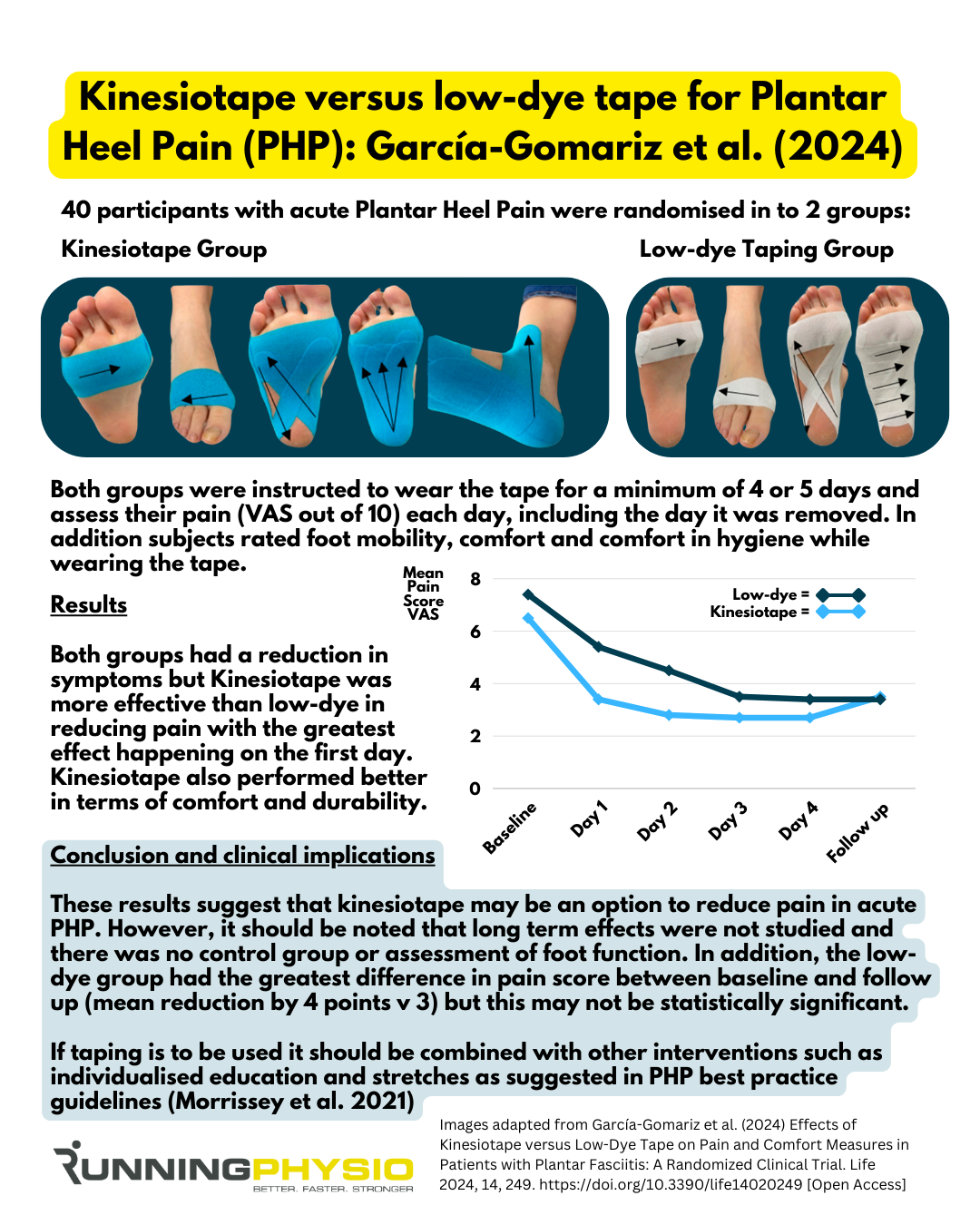
It does seem that both taping strategies may help reduce acute pain in PHP. Kinesiotaping appears to get results more rapidly, but as I mentioned in the graphic, the overall pain reduction from baseline was very slightly larger in the low-dye group. This isn’t really mentioned in the study, so it’s not clear if this would be considered statistically significant or clinically meaningful.
I say may reduce pain, as without a control group, we can’t be certain if symptoms simply changed over time (as they often do, especially in acute presentations).
I’d also add that there are multiple ways to tape the foot for Plantar Heel Pain, and this study only compares two. Podiatrist Simon Bartold, founder of Bartold Clinical, shared a video of his taping technique. He’s quite specific about the approach, position of the foot and level of support needed. Note how different this is from the technique in Dr Kevin Kirby’s video. Both are experts in their field and hugely experienced.
I appreciate these videos may be a little dated now, but they do show that ‘low-dye taping’ may look very different in the hands of one clinician versus another, so we need to be careful in generalising the results of this study.
Taping is not without controversy, especially kinesiotape, which was applied in this study. I can’t claim to be an expert in it. A brief literature review reveals an abundance of research with this tape being used to treat pain, swelling, proprioception, muscle strength and more.
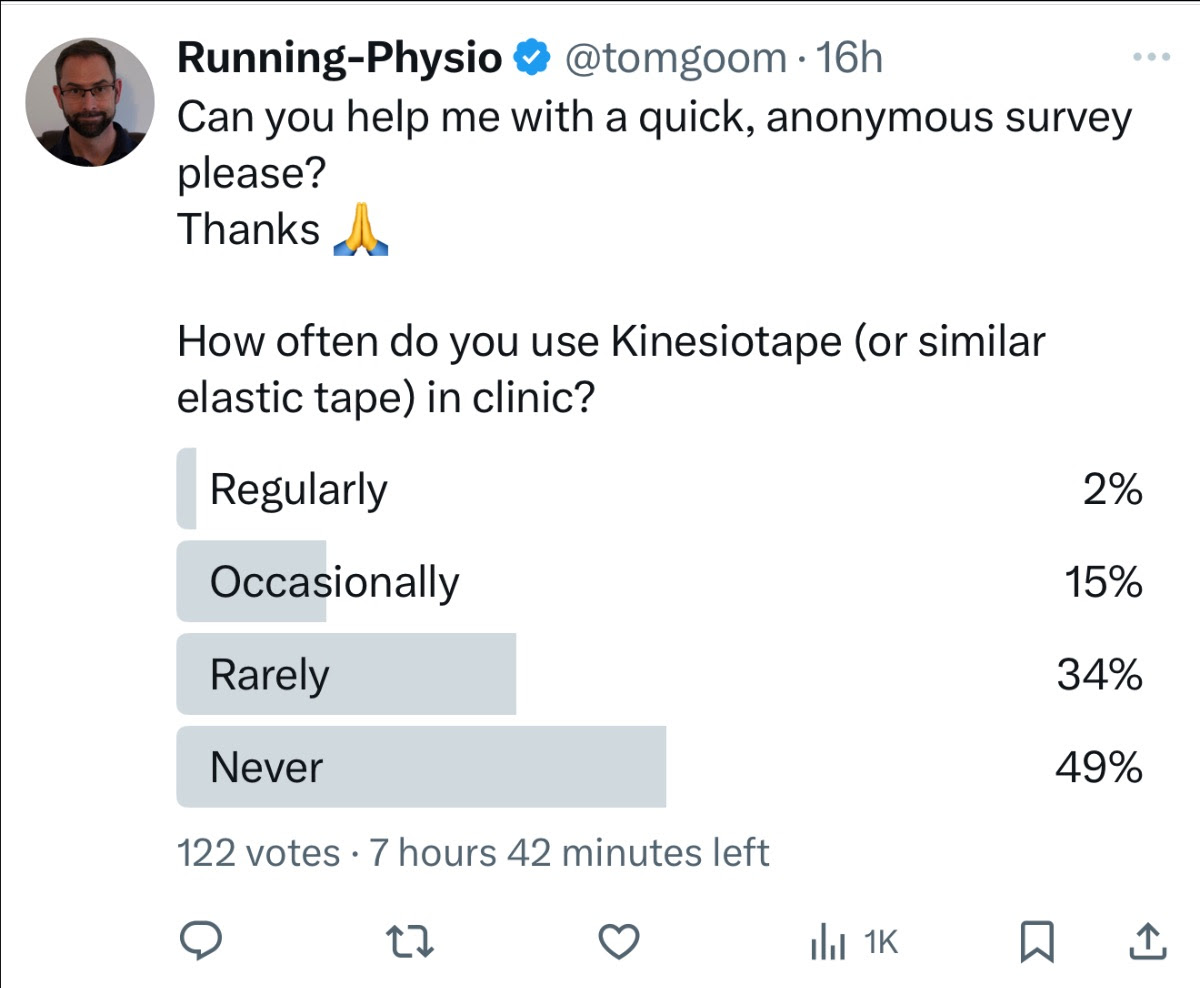
However, whether it’s actually effective in any of these roles is certainly questionable. I think many clinicians view it as a colourful placebo, which may be why nearly half of my followers that I surveyed on X say they never use it:
Previous systematic reviews, such as Parreira et al. (2014), have suggested that current evidence does not support the use of kinesio taping in clinical practice. I did find a more recent review, Tran et al. (2024), with more positive findings, but I’m yet to analyse this in any detail, so I’d recommend reading it in full before making any conclusions.
Clinical implications and bigger picture
When the aim is to reduce pain in the short term, tape seems a very reasonable option to consider. The choice of which type of tape will come down to the individual and what their goals and needs are. We also need to bear in mind that some people are allergic to certain tapes, so this should be checked before application.
If more physical support is needed, then low-dye is more likely to achieve this due to its more rigid nature. It doesn’t appear to be as comfortable or durable as elastic tape, though, so may be better suited to short-term usage (e.g. during sport/ provocative activity). However, runners and athletes will sweat during sport and in my experience, this can cause more rigid tape to come off. In practice, it’s usually best to try different options during training to see what works and can be applied if needed during competition.
If comfort and mobility are priorities (or rigid tape comes off during sport), then elastic tape may be preferable. If it’s well tolerated and especially effective for symptoms, we may suggest using it for up to 4 days or consecutive applications (e.g. every 3 or 4 days). Dr Smith mentions this in her podcast, and she recommended a period of time without tape between applications (e.g. overnight) to avoid skin irritation.
Recent best practice guidelines (Morrissey et al. 2021) support the use of tape combined with education and stretches. Koc et al. (2023) suggest tape (either rigid or elastic) is used in conjunction with other treatments for short-term improvements in pain and function, and this is how I would tend to use it in clinic.
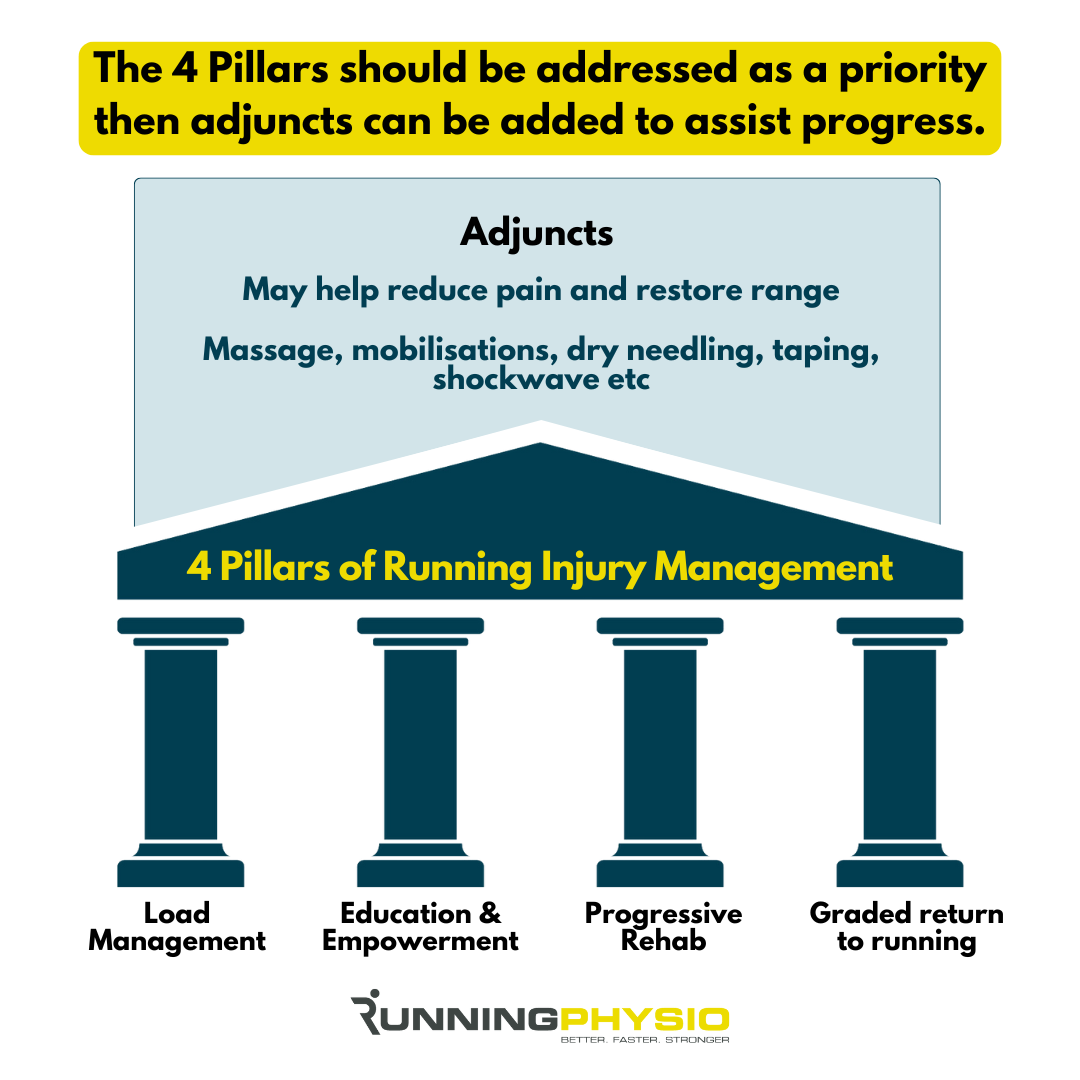
I view tape as an optional ‘adjunct’ to our main strategies for managing running injury, ‘The 4 pillars’ (below). These strategies need to be in place first as a priority, then we can consider adjuncts that might reduce pain or improve range or movement quality:
One more snippet on this that I wanted to share comes from the Morrissey et al. (2021) best practice guide, where some of the experts interviewed for the paper used taping to predict if foot orthoses may be helpful:
“If I tape them and their symptoms decrease, and then I can say—okay, I think I can replicate what the tape is doing with either shoes or orthoses.” Expert 13, Morrissey et al. (2021).
In conclusion, tape can be useful as a short-term strategy to reduce pain or modify load, but I’d be thinking about long-term options to restore capacity and return people to their chosen sport without needing to be strapped up!










