Our articles are not designed to replace medical advice. If you have an injury we recommend seeing a qualified health professional. To book an appointment with Tom Goom (AKA ‘The Running Physio’) visit our clinic page. We offer both in-person assessments and online consultations.
UKRunchat blogger and top podiatrist Nick Knight’s joins us again for Part 2 in his series on blogs on orthoses. Part 1 tackled what orthoses are and how they’re used, next up is the tricky matter of how orthoses actually work…
Follow Nick on Twitter via @NKSportsPod
The truth about how orthoses work is we are not 100% sure, we have different models and theories. To answer this question we need to understand patient and treatment goals, is it pain relief, running quicker for longer, or, in a diabetic patient, reducing the risk of ulceration?
We know that they do work and we have plenty of evidence to back this up (e.g Moen et al. 2009, Loudon and Dolphino 2010, Yeung et al. 2011)
Do orthoses work all the time? No.
Do need to wear orthoses all of the time? No.
Orthoses are just like any other type of treatment, it is about getting the correct treatment for that patient. In a way orthoses can be related to physiotherapy (in the context of the patient can attend my clinic and they have not brought the orthoses to the appointment with them) I can have a patient come see to see me who has had physiotherapy, however I do not know what treatment. Is it stretching, a loading program, taping or massage? This information is important and necessary to know before treatment. This is similar to Orthoses, in that the healthcare professional needs to know the material type, prescription, stiffness etc in order to get a complete idea of their treatment.
I hear in my clinic on a weekly basis that patients have been prescribed orthoses in the past in order to correct their alignment which shall reduce pain, the idea that Orthoses can help with this is a myth and not true.
A bit of science now, when we talk about ‘straightening’ people up this is referring to what is known as kinematics. Kinematics is the study of movement and angles, and in simple terms, the visual changes we can see. To have a successful treatment outcome we do not have to change kinematics, however this does not mean that they’re not important.
A second, important consideration is the effect of the orthoses on kinetics. Kinetics is the study of forces acting on an object. Forces (kinetics) can change despite no visible change in movement (kinematics). There are a couple of ways of visualising this; one is to lean against the wall with one hand, now push slightly harder and you’ll see no visual change in the movements within the arm and the wrist, however the force applied to the wall is greater. The other way is to stand on a flat surface, now stand on the edge of a step making sure your heel remains horizontal, your heel position is visually in the same position regardless of if you’re standing on the edge of a step or a flat surface however the forces going through the calf muscle are completely different;
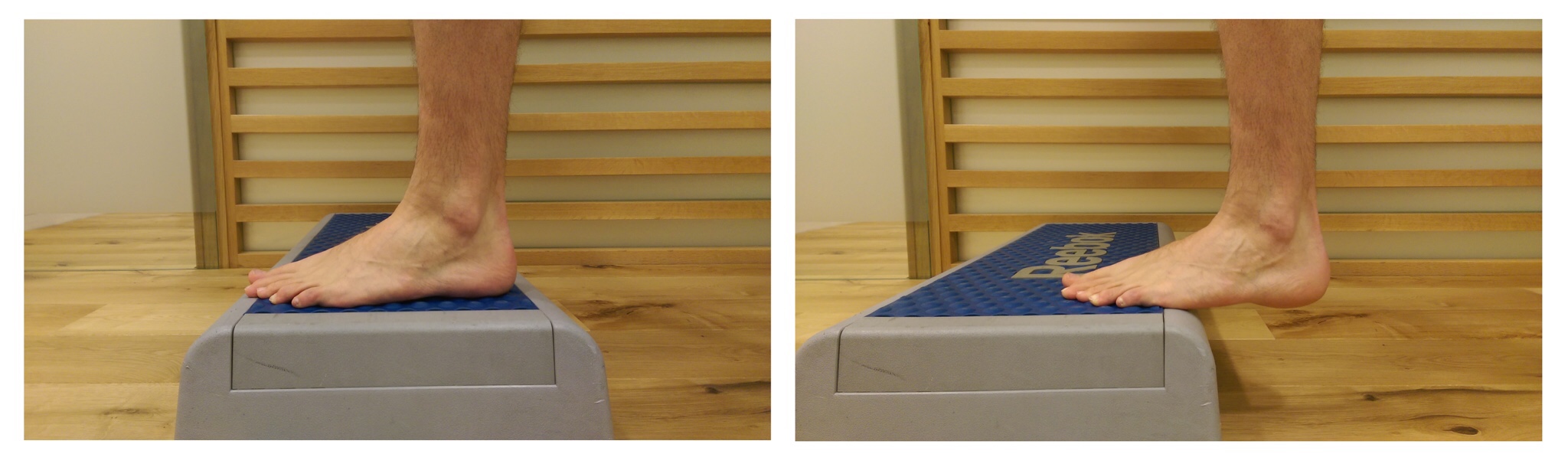
Picture source Ian Griffiths blog on mechanics
The point being that we can have a kinetic effect without changing the kinematics and this can often lead to a positive treatment outcome, the issue we have is how do we measure the kinetics in clinic? If we can’t actually see kinetic changes they can be hard to assess and quantify and challenging to study scientifically. One of the biggest issues we have with the research regards to orthoses is that every person reacts differently to them and there is no way of predicting how one person will react compared to another, to put this into context if you are trying to compare orthoses to drugs and you to put them into a trial you would have to give every different participant in the trial a different dosage of the drug, making the trial flawed from day one.
It is also important to remember the psychological effect orthoses can have and how can we quantify this in research, runners can sometimes feel vulnerable without using the orthoses. It could be argued that we know orthoses are not causing any harm or weakening muscles so if the patient feels they are offering some benefits why remove them?
I still hear from time to time that orthoses weaken the foot and surrounding leg muscles, this is not true. I am yet to find any studies that back this claim up, yet there are many studies showing muscle activity remains the same.
Then there’s also the neuromotor effects orthoses have on the body and this area of research is growing. There was a good paper in the British Journal of medicine showing that orthoses reduced the frequency of falls within an elderly population, but again and how can we measure the neuromotor effects in most standard clinics?
Looking at all this information, you can appreciate that whilst we know orthoses work, the reason why they work we are not sure of and moreover the reason may be different for different people.
In one of my clinics we can use in-shoe pressure analysis and 3D gait analysis to help with orthoses prescription, however not many clinics in the country have access to this type of technology. It is important to know what to do with the data, i.e. treat the patient not the scan, as there is no definition of normal function. It is important to look at the big picture and look at function with and without orthoses, whilst trying to problem solve differences and consider if orthoses are the answer or not.
Coming up in part 3 – which are best custom orthoses or ‘off the shelf’ and how are orthoses prescribed?…










[…] Orthoses – so much more than ‘fit and forget’ Part 2 – by Nick Knight […]
How do you think about orthoses for children with flatfeet? I had a patiënt in my clinic who’s 12 years old and wears orthoses since he’s 4!!! He had medial knee pain even with the orthoses. The parents told me that the gait pattern even got worse from 7-11 year.
I think children should do excercises for their flat feet to have a future life without orthoses from the age of 16-18. This could be in combination with orthoses.
Looking forward to part 3 🙂
Bernard:
Please tell me why a 12 year old with a nearly full grown foot would want to not wear their foot orthoses if they are indeed helping them. I have seen hundreds of children in this age group that wear foot orthoses into adulthood without any problems. Would you also recommend that 12 year olds who wear prescription eyeglasses or contact lenses should do “eye exercises” for their Imperfect eyesight to that they can “have a future life” without eyeglasses or contact lenses “from the age of 16-18”?
Sorry, there is absolutely no research evidence to suggest that the long-term wearing of foot orthoses causes any pathologies or weakness of the foot and/or lower extremity, contrary to what is written so often by ill-informed clinicians and individuals on the internet. I have been wearing prescription foot orthoses on a daily basis for the past 40 years, since the age of 19, and they have only helped me, not hurt me.
Bernard, why would you want to take away a good pair of well-fitting and function custom foot orthoses from an individual any more than you would want to take away a good pair of custom eyeglasses or contact lenses from another individual?
Dr. Kirby
**************************************************
Kevin A. Kirby, DPM
Adjunct Associate Professor
Department of Applied Biomechanics
California School of Podiatric Medicine at Samuel Merritt College
E-mail: [email protected]
Website: http://www.KirbyPodiatry.com
Private Practice:
107 Scripps Drive, Suite 200
Sacramento, CA 95825 USA
Voice: (916) 925-8111 Fax: (916) 925-8136
***************************************************************************
Hi Bernard,
Orthoses and children is always a difficult subject. Not all children I see with a flexible pes planus will get orthoses.
For example if they have a flexible pes planus, however can play their sport pain free and there is not family history of foot realted pain then I tend to apply the watchful wait approach.
However if there is pain for a family hisotry of pain then I may issue orthoses, with the advice that they may not be needed, however if the orthoses are comfortable (rule number 1) then have no issues children uing them, as they are not casuing any weakening of muscles.
With reagards to your knee pain patient, I even in children look further up the chain, if they are active then look a proximal control and hip postition, at 12 they my still be internally rotated still, with poor gluteal function.
The foot will do want it will want to do when growing with or with out orthoses. Some people have the impression that orthoses will make the foot grow an arch, wrong.
I have copied a reference below, for a nice paper about children and orthoses.
Evans AM. The flat-footed child — to treat or not to treat: what is the clinician to do? J Am Podiatr Med Assoc. 2008; 98(5):386-93
Nick:
Another good article.
I agree with you that the key to understanding the therapeutic benefits of foot orthoses is to try to more firmly grasp the changes in external and internal forces and moments (i.e. kinetics) that foot orthoses can produce in the feet and lower extremities of our patients. By altering the specific locations, magnitudes and temporal patterns of ground reaction forces (i.e. external forces) acting on the plantar foot, foot orthoses have the unique ability to alter the internal forces and moments acting within the joints, tendons, ligaments, cartilage, bones and fascia that constitute the structural elements of the foot and lower extremity. This fact is very significant due to unusually magnitudes of forces acting on the feet during weightbearing activities. In addition, what foot orthoses can do for our patiens is often something that simply can’t be accomplished by any amount of strengthening, stretching or other physical therapy measures.
The ability of well-designed foot orthoses to alter the stresses acting within the structural components of the foot and lower extremity allow orthoses to not only reduce the pathological magnitudes of stresses that are causing the injuries of our patients, but also can function to improve the gait function (i.e. improve their gait kinematics) and prevent further injury. The clinician with a good understanding of foot orthosis biomechanics and foot and lower extremity kinematics and kinetics should be able to utilize the specific orthosis design parameters which will optimize the function and therapeutic effectiveness of the prescription foot orthoses for their patients.
The days of thinking that foot orthoses “realign the skeleton” are over. Now, we must pursue the theoretical and practical research that will allow us to better understand the Direct Mechanical and Neuromotor effects of foot orthoses. http://www.podiatry-arena.com/podiatry-forum/showthread.php?t=22890
Keep up the great writing, Nick!
Cheers,
Kevin
**************************************************
Kevin A. Kirby, DPM
Adjunct Associate Professor
Department of Applied Biomechanics
California School of Podiatric Medicine at Samuel Merritt College
Private Practice:
107 Scripps Drive, Suite 200
Sacramento, CA 95825 USA
Voice: (916) 925-8111 Fax: (916) 925-8136
**************************************************
[…] podiatrist Nick Knight is back with the final instalment! Having covered what orthoses are and what they do it's on the tricky question of how they are […]
Comments are closed.